Key Takeaways
- Clinical Bottom Line
- The modern answer is not dry. It is deliberate.
- WATERFALL changed the hydration conversation
- What the 2024 ACG guideline clarifies for real-world care
Clinical Bottom Line
| Early-management question | 2026 practical answer |
|---|---|
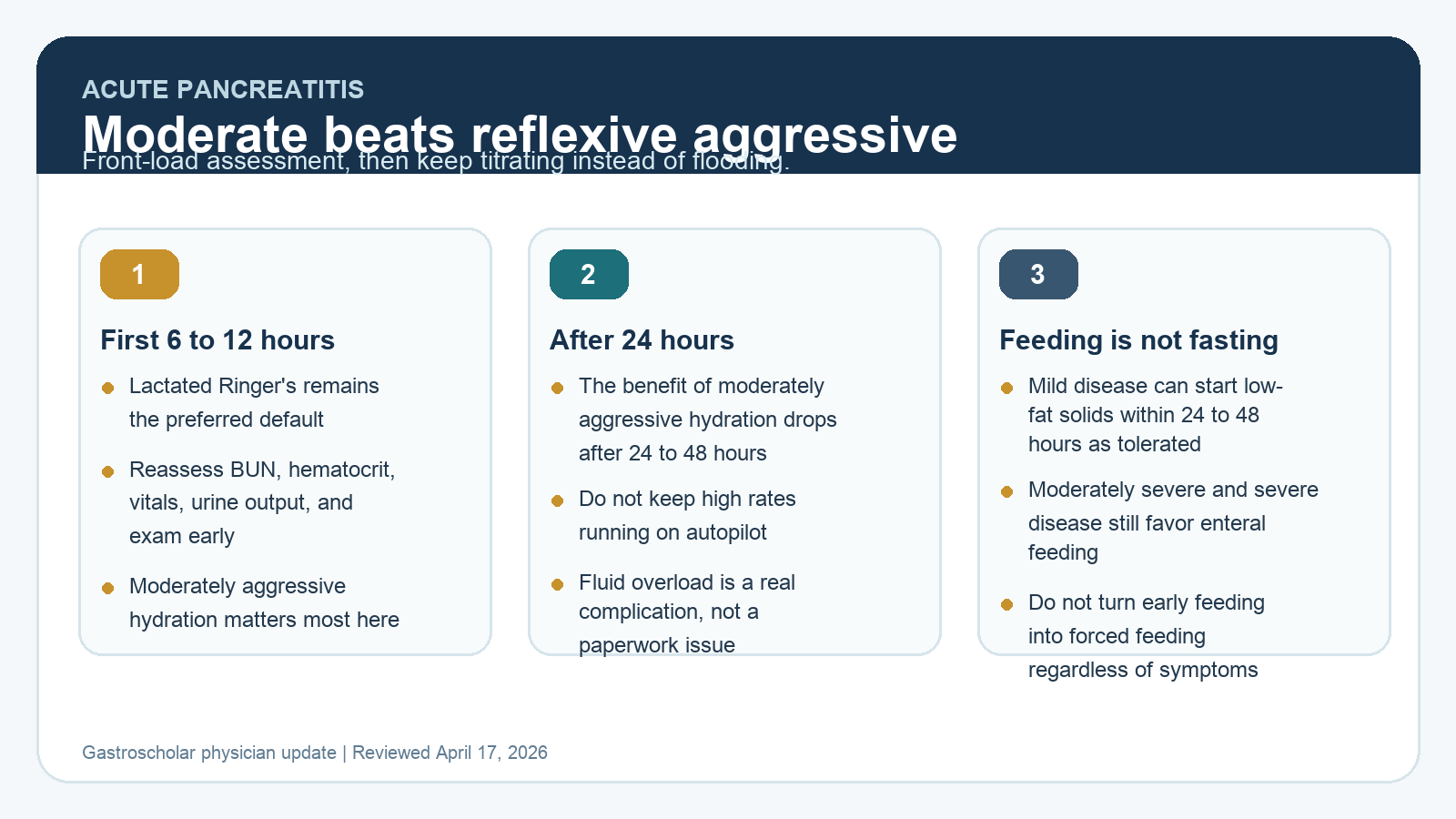
| Which IV fluid? | Lactated Ringer’s remains the preferred default crystalloid in most patients. |
| How much fluid up front? | Think moderately aggressive hydration in the first 6 to 12 hours with frequent reassessment, not automatic flooding. |
| What about after day 1? | Hydration strategy should be reassessed closely. ACG highlights note little benefit from moderately aggressive hydration after 24 to 48 hours. |
| When can mild cases eat? | Within 24 to 48 hours with a low-fat solid diet as tolerated. “As tolerated” still matters. |
| What about moderately severe or severe disease? | Prefer enteral nutrition, often via NG tube, and avoid parenteral nutrition if possible. |
The modern answer is not dry. It is deliberate.
Modern fluid management is sometimes oversimplified as “stop giving a lot of fluid.” That misses the real shift. Current care still emphasizes early resuscitation. What changed is the target. The goal is no longer indiscriminate flooding. It is moderately aggressive hydration early, paired with close reassessment.
That distinction matters because undertreating true volume depletion is still dangerous, especially in the first hours. The updated ACG framing is practical: monitor closely in the first 6 to 12 hours, use lactated Ringer’s, and keep checking vitals, BUN, and hematocrit as the patient’s trajectory declares itself.
WATERFALL changed the hydration conversation
The biggest practice-changing trial remains WATERFALL. In that randomized trial, aggressive fluid resuscitation caused more fluid overload than a moderate strategy without improving clinical outcomes. Fluid overload developed in 20.5% of aggressively resuscitated patients versus 6.3% in the moderate group, and the aggressive strategy did not reduce moderately severe or severe pancreatitis.
That trial did not prove that fluids are unimportant. It showed that reflexively pushing more fluid is not the same thing as better care.
What the 2024 ACG guideline clarifies for real-world care
The 2024 ACG guideline highlights are helpful because they translate the post-WATERFALL mindset into bedside workflow.
- Lactated Ringer’s is preferred.
- Moderately aggressive hydration matters most in the first 6 to 12 hours.
- The benefit of that strategy falls after 24 to 48 hours.
- Reassessment, not autopilot, is the core behavior.
That is the part busy doctors actually need. The question is not whether fluids are “aggressive” or “conservative” in the abstract. The question is whether the rate still fits the patient 6 hours later.
The newer meta-analysis points in the same direction
A 2024 meta-analysis of 6 randomized trials also favored moderate over aggressive replacement. Across 632 patients, aggressive fluid therapy was associated with higher all-cause mortality and did not improve the major secondary outcomes the authors examined. That result should not be used as permission to under-resuscitate sick patients, but it does strengthen the case against routine early flooding.
Early feeding means “as tolerated,” not “regardless of symptoms”
Early feeding is also easy to overstate if it gets reduced to “start solids no matter what.” That is not how the current guidance reads.
For mild disease, ACG supports early oral feeding with a low-fat solid diet within 24 to 48 hours as tolerated. If the patient is nauseated, vomiting, severely distended, or clearly not ready, forcing intake is not the point. In moderately severe or severe disease, enteral nutrition remains preferred, often by NG tube, while parenteral nutrition should be avoided if possible.
A practical first-48-hours protocol
| Time window | What to do |
|---|---|
| Arrival to 6 hours | Assess hemodynamics and severity risk, start lactated Ringer’s, and watch BUN, hematocrit, urine output, respiratory status, and exam rather than a fixed-volume script. |
| 6 to 12 hours | This is the main window where moderately aggressive hydration matters most. Reassess whether the patient still looks volume responsive. |
| 24 hours | If mild disease is settling and nausea or vomiting are not limiting, start a low-fat solid diet instead of waiting for a pain score of zero. |
| 24 to 48 hours | Move away from reflex escalation. Continued moderate hydration has diminishing value if the patient is no longer clearly volume depleted. |
| Moderately severe or severe disease | Use enteral feeding rather than parenteral nutrition whenever possible, and keep the rest of management focused on complications and organ support. |
What not to do in 2026
- Do not equate “modern” with under-resuscitating the patient on arrival.
- Do not keep pushing high fluid rates after 24 hours just because that was the opening plan.
- Do not write “feed early” as if nausea, vomiting, ileus, and tolerance no longer matter.
- Do not let the hydration debate distract from severity assessment, complication monitoring, and enteral nutrition.
Selected references
- ACG Guideline Highlights: Management of Acute Pancreatitis. 2024.
- Aggressive or Moderate Fluid Resuscitation in Acute Pancreatitis. N Engl J Med. 2022.
- Aggressive Versus Moderate Fluid Replacement for Acute Pancreatitis: An Updated Systematic Review and Meta-Analysis. JGH Open. 2024.
- Diagnosis and Management of Acute Pancreatitis. Gastroenterology. 2024.
Last reviewed April 17, 2026. This update is written for clinicians who want a realistic fluid and feeding protocol for the first 48 hours of acute pancreatitis.