Key Takeaways
- Clinical Bottom Line
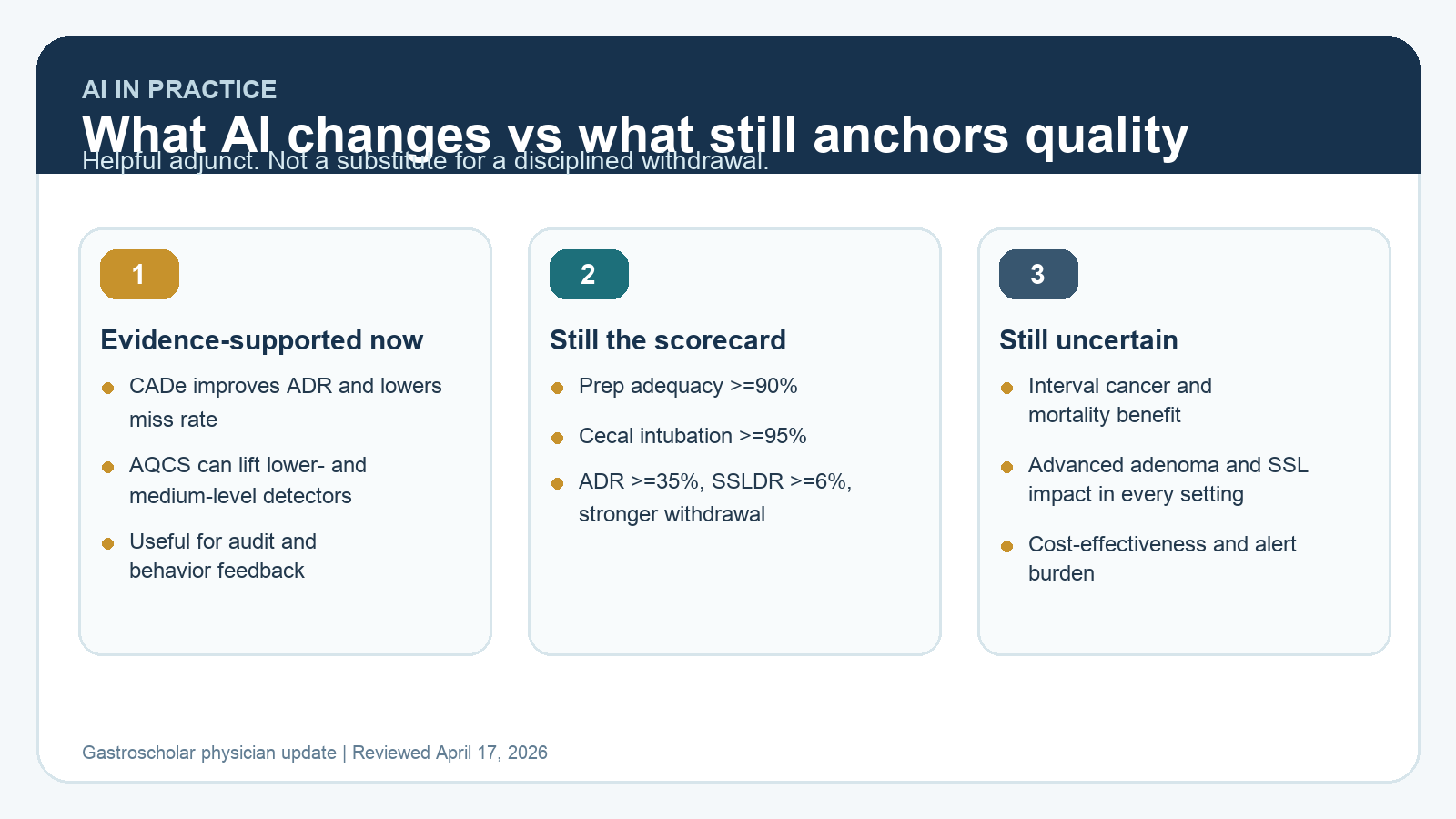
- AI has not replaced standard quality metrics
- First, separate CADe, CADx, and CAQ
- What is established in 2026
Clinical Bottom Line
| Question | What the current evidence supports |
|---|---|
| Should every unit adopt CADe? | Not as a universal standard. In March 2025, AGA made no recommendation for or against CADe-assisted colonoscopy because long-term patient-important benefit remains uncertain. |
| Is CADe useless? | No. Randomized data consistently show more adenoma detection and lower adenoma miss rates with CADe. |
| What still defines quality? | Prep adequacy, cecal intubation, withdrawal technique, ADR, SSLDR, complete resection, and documentation still define colonoscopy quality in 2026. |
| Are AI quality-control tools ready for prime time? | Promising, but not yet accepted as stand-alone society benchmarks. They should augment, not replace, standard quality indicators. |
| What is the practical takeaway? | Use AI as an adjunct to improve lesion detection and procedural discipline, but do not confuse software alerts with proof of a high-quality examination. |
AI has not replaced standard quality metrics
CADe improves detection. CAQ systems that monitor withdrawal behavior, blind spots, or fold exposure are increasingly credible. But current society guidance still treats AI as an adjunctive technology, not as a replacement for established quality metrics or expert endoscopic judgment.
First, separate CADe, CADx, and CAQ
- CADe: computer-aided detection. Real-time alerts for possible lesions.
- CADx: computer-aided diagnosis or characterization. Optical prediction support.
- CAQ: computer-aided quality or quality-control systems. These monitor withdrawal time, fold exposure, blind spots, luminal coverage, or cleaning behavior.
Most of the strongest evidence remains on CADe. CAQ is promising, but the evidence base is newer and less standardized.
What is established in 2026
Randomized evidence continues to show that CADe improves detection metrics. A 2024 meta-analysis of randomized controlled trials reported a 20% relative increase in adenoma detection rate and a 55% reduction in adenoma miss rate with AI-assisted colonoscopy. That matters, especially because missed lesions remain a major pathway to post-colonoscopy colorectal cancer.
At the same time, AGA issued a deliberately conservative 2025 guideline: no recommendation for or against CADe-assisted colonoscopy. That is not indecision. It reflects a real evidence gap between better short-term lesion detection and proven downstream benefit on advanced neoplasia, interval cancer, mortality, cost-effectiveness, and workflow burden.
Why the U.S. and ESGE positions differ
The most interesting 2025 development is that North American and European society positions are not identical.
- AGA 2025: no recommendation for or against CADe in adults undergoing colonoscopy.
- ESGE 2025: weak recommendation favoring CADe for well-informed patients who have already chosen colonoscopy for screening or surveillance.
That split tells clinicians something useful. The technology has enough signal to merit real adoption discussions, but not enough certainty to become a mandatory quality requirement across all practices.
The quality indicators that still matter most
Current quality measurement is still anchored in the 2024 ACG/ASGE colonoscopy indicators, not in proprietary AI dashboards. The highest-yield scorecard still includes:
- Bowel prep adequacy >=90%.
- Cecal intubation rate >=95%.
- ADR >=35% in adults older than 45 years undergoing screening, surveillance, or diagnostic colonoscopy.
- SSL detection rate >=6%.
- Longer and methodical average withdrawal time in normal examinations, closer to 8 minutes rather than the older 6-minute floor.
- High-quality resection and documentation.
AI does not make these indicators obsolete. It helps some endoscopists reach them more reliably, but the benchmark itself is still built on classic colonoscopy fundamentals.
Where AI quality-control systems are most believable
CAQ systems are the most interesting frontier because they target behavior, not just lesion alerts. A 2025 randomized clinical trial of an automatic quality control system showed higher nonadvanced adenoma detection in the AI-assisted group versus standard colonoscopy (30.1% vs 21.2%), with the clearest gains among lower- and medium-level detectors. That is encouraging because the biggest public-health opportunity is often lifting the floor, not marginally improving elite detectors.
Earlier work also supports the concept biologically. In a 2022 study, an AI-based fold examination quality system correlated strongly with expert assessment, historical ADR, and withdrawal time. That is the kind of signal that makes CAQ worth watching. But these systems still need broader validation across diverse equipment platforms, practice settings, and endoscopist skill levels before they can be treated as universal benchmarks.
What AI still does not prove
- That the exam prevented cancer.
- That the most clinically meaningful lesions, especially advanced adenomas and sessile serrated lesions, were preferentially improved enough to change long-term outcomes.
- That alert-heavy systems are cost-effective in every practice environment.
- That an acceptable AI dashboard compensates for poor washing, poor distention, rushed withdrawal, or incomplete resection.
A practical 2026 workflow for using AI without fooling yourself
| Use AI for this | Do not let AI replace this |
|---|---|
| Real-time lesion prompting during withdrawal | Cleaning, distention, fold exposure, and position changes |
| Feedback to lower-performing detectors | Benchmarking against ADR, SSLDR, cecal intubation, and adverse events |
| Audit support for withdrawal technique | Thoughtful characterization, resection planning, and pathology-informed surveillance |
| Unit-level quality improvement | Believing that software certification equals a high-quality colonoscopy |
Selected references
- AGA Clinical Practice Guideline on CADe-assisted colonoscopy. 2025.
- ESGE Position Statement on CADe colonoscopy in CRC screening and surveillance. 2025.
- Rex DK, et al. Quality indicators for colonoscopy. Gastrointest Endosc. 2024.
- 2024 meta-analysis of randomized CADe trials in colonoscopy.
- Liu J, et al. Automatic Quality Control System and Adenoma Detection Rates During Routine Colonoscopy. JAMA Netw Open. 2025.
- Xie Y, et al. AI-based assessment of colonoscopic withdrawal technique and fold examination quality. Endoscopy. 2022.
- Corley DA, et al. Adenoma detection rate and risk of colorectal cancer and death. N Engl J Med. 2014.
Last reviewed April 17, 2026. This review is written for clinicians deciding how to interpret AI assistance inside real colonoscopy quality programs.