Key Takeaways
- Clinical Bottom Line
- PEP prevention is a bundle, not a single trick
- What the ASGE guideline still tells us
- The 2024 trial changed how to talk about indomethacin alone
Clinical Bottom Line
| Prevention step | 2026 practical answer |
|---|---|
| Rectal NSAIDs | Give rectal indomethacin 100 mg to most adults undergoing ERCP unless contraindications such as recent peptic ulcer disease or significant renal insufficiency are present. |
| Cannulation strategy | Wire-guided cannulation is preferred over contrast-guided cannulation to reduce PEP risk. |
| High-risk pancreatic duct access | Do not rely on NSAIDs alone when the pancreatic duct has been repeatedly or deeply accessed. Prophylactic pancreatic stenting still matters. |
| Hydration | Aggressive lactated Ringer’s hydration remains reasonable in selected patients if heart failure, renal insufficiency, or advanced liver disease are not limiting factors. |
| Best mental model | PEP prevention is a bundled strategy, not a single suppository. |
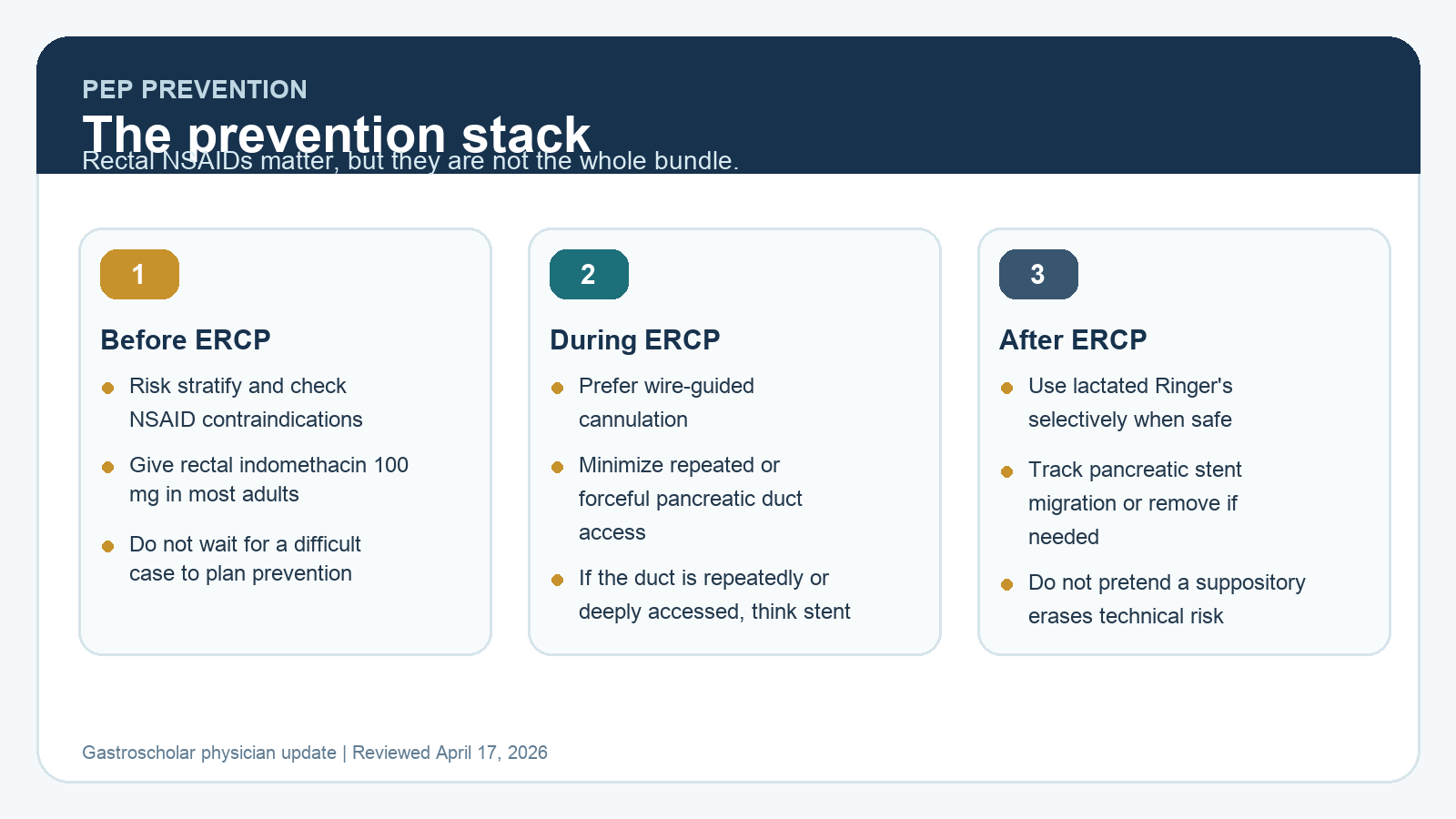
PEP prevention is a bundle, not a single trick
Rectal indomethacin remains a core part of prevention, but current practice is broader than a single-drug strategy. Post-ERCP pancreatitis prevention works best when the endoscopist treats it as a layered protocol that starts before cannulation, continues during the procedure, and does not ignore post-procedure physiology.
Busy doctors do not need another dramatic reminder that PEP is serious. They need a practical stack they can apply consistently.
What the ASGE guideline still tells us
The 2023 ASGE guideline remains the main U.S. procedural framework.
- Use preprocedural rectal NSAIDs for unselected ERCP patients and for high-risk patients, with indomethacin 100 mg as the standard adult dose.
- Prefer wire-guided cannulation over contrast-guided cannulation.
- Place a prophylactic pancreatic stent in high-risk patients when the pancreatic duct has been repeatedly or deeply accessed, and consider it more broadly in high-risk patients when duct access is easy.
- Use aggressive lactated Ringer’s hydration selectively when cardiorenal or hepatic limitations do not make that unsafe.
That structure matters because it prevents the common mistake of treating NSAIDs as a reason to relax on technique.
44% preview unlocked
Unlock the rest of this physician update
Enter your email to keep reading "Post-ERCP Pancreatitis Prevention in 2026: Rectal NSAIDs, Pancreatic Stents, and Practical Risk Reduction" and get practical GI endoscopy updates from GastroScholar.
- Immediate access to the rest of this article
- Practical endoscopy notes for busy doctors
- One unlock covers the rest of the gated pilot posts on this browser