GastroScholar Magazine
The Modern Journal for GI Innovation
Daily reporting on endoscopy, clinical evidence, and practice-changing advances in gastroenterology.
Editor's Picks
Cold Snare Polypectomy for Sub-10 mm Polyps in 2026: Where CSP Is Standard and Where It Is Not
A practical update on cold snare polypectomy for diminutive and small colorectal polyps, including technique, when hot resection is still...
EUS-Guided Gastroenterostomy for Malignant Gastric Outlet Obstruction in 2026: Where It Fits Between Stenting and Surgery
A practical clinician update on EUS-guided gastroenterostomy for malignant gastric outlet obstruction, including when it outperforms enteral stenting, when surgery...
AI in Colonoscopy Quality: What CADe Changes and What Still Depends on the Endoscopist
A clinician-focused review of CADe, AI quality-control systems, and the quality indicators that still define a good colonoscopy in 2026.
Just In
-
Cold Snare Polypectomy for Sub-10 mm Polyps in 2026: Where CSP Is Standard and Where It Is Not
-
Endoscopy Sedation in 2026: Propofol, Capnography, and When Anesthesia Support Is the Safer Plan
-
AI in Colonoscopy Quality: What CADe Changes and What Still Depends on the Endoscopist
-
IBS-D Biomarkers in 2026: Positive Diagnosis, Fecal Calprotectin, and When Colonoscopy Still Matters
-
Chronic Hepatitis B in 2026: EASL 2025, Functional Cure, and What Still Belongs in Practice
-
The 2026 Frontiers: Robotic Endoscopy and Cryoballoon Efficacy
-
EUS-Guided Drainage of Peripancreatic Fluid Collections in 2026: When To Drain, When To Wait, and When Percutaneous Still Matters
-
Cold Snare Polypectomy for Sub-10 mm Polyps in 2026: Where CSP Is Standard and Where It Is Not
A practical update on cold snare polypectomy for diminutive and small colorectal polyps, including technique, when hot resection is still reasonable, and what current guidelines say about clipping and forceps.
Top Stories
Trending in GI Research
-
The 2026 Frontiers: Robotic Endoscopy and Cryoballoon Efficacy
-
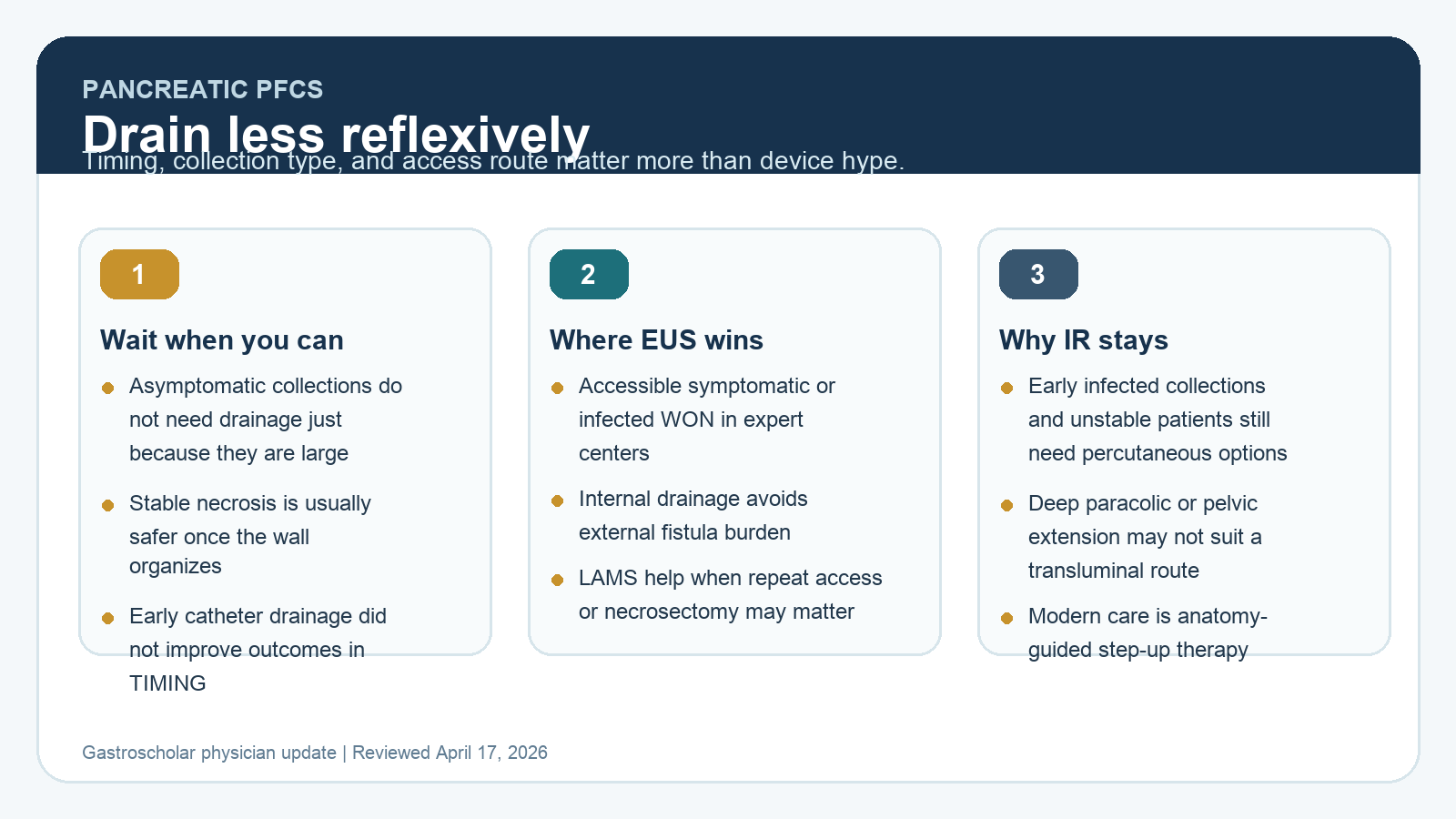
EUS-Guided Drainage of Peripancreatic Fluid Collections in 2026: When To Drain, When To Wait, and When Percutaneous Still Matters
-
Gastric Functional Zones: The Fundus vs. Antrum Dynamics
-
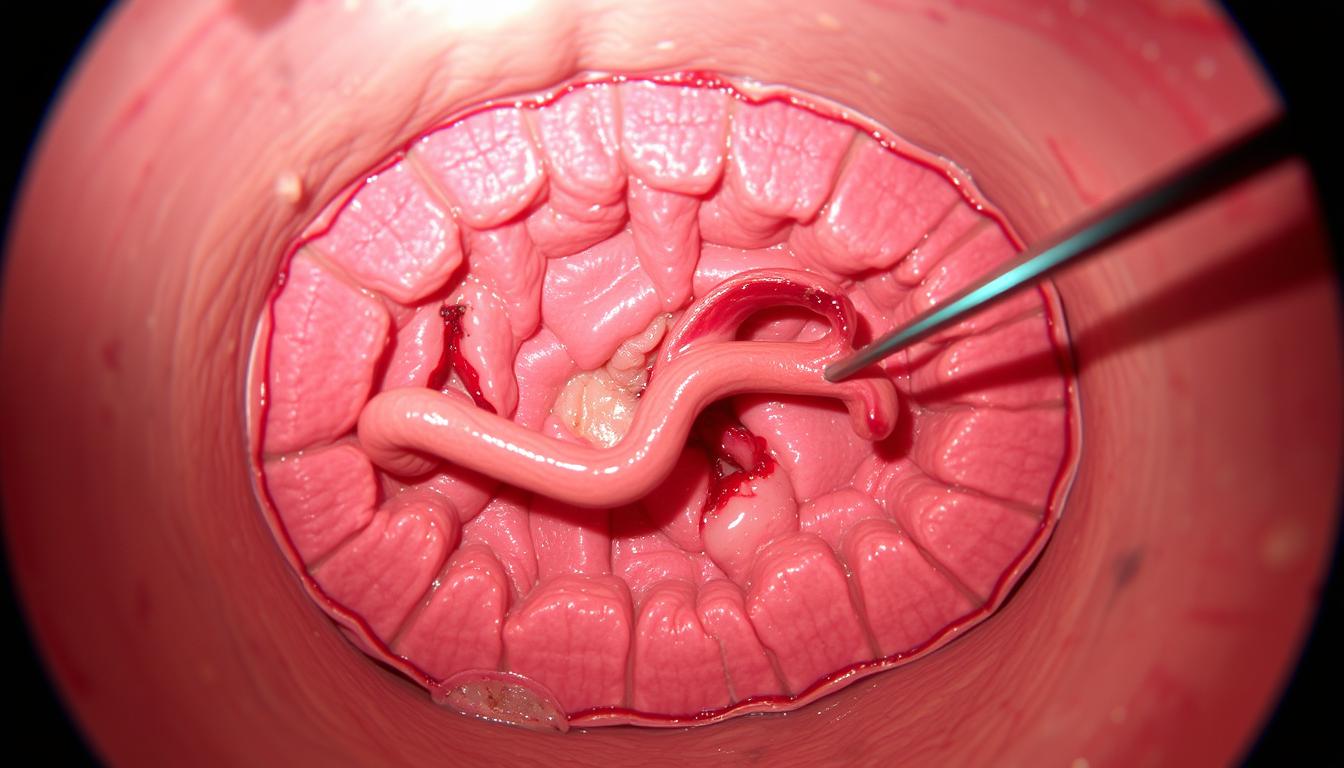
Dieulafoy’s Lesion: The Exoluminal Arterial Blowout
-
Slim Therapeutic Gastroscopes (9.2mm) in Difficult Anatomies
-

Accessories for Upper Esophageal Sphincter (UES) Interventions
Latest from the Archive
-

Colorectal Screening vs. Diagnostic Colonoscopy Triage
Clinical Bottom Line Endoscopic Categorization Defining Criteria Core Intent Screening (Preventative) Asymptomatic, average-risk patient (Age ≥ 45). To find and…
-

Propofol Half-Life and Post-Sedation Neurocognition (2026)
Clinical Bottom Line Pharmacological Agent Context-Sensitive Half Time Discharge Implication Propofol < 10 minutes. Immediate physical awakening, but subtle neurocognitive…
-

Aspiration Risk and NPO Guidelines for Deep Sedation
Clinical Bottom Line Dietary Content Required Fasting Duration (ASA) Gastric Emptying Physiology Clear Liquids (Water, Apple Juice) 2 Hours prior…
-

Post-Procedural Positioning for Flatus and Comfort
Clinical Bottom Line Insufflation Gas Absorption Rate Positioning Requirement Carbon Dioxide (CO2) Absorbed 160x faster than room air into the…
-

Avoiding Split-Dose Bowel Prep Failures
Clinical Bottom Line Preparation Element Modern Protocol Standard Failure Implication Split-Dosing (The Rule) 50% taken the evening before; 50% taken…
-

Caffeine and Vasodilation Post-Sedation
Clinical Bottom Line Dietary Agent Physiological Effect Post-Endoscopy Implication Caffeine (Coffee/Tea) Mild diuretic and systemic stimulant. Safe after standard procedures;…
-

Post-Colonoscopy Diet: Recovery From Aggressive Lavage
Clinical Bottom Line Procedural Status Immediate Post-Op Diet Delayed Restrictions Diagnostic (No Polyps Removed) Return to normal diet immediately upon…
-

Cardiopulmonary Complications During Endoscopy
Clinical Bottom Line Complication Pathophysiology Immediate Countermeasure Hypoxia / Apnea Loss of respiratory drive vs. upper airway mechanical obstruction. Jaw…
-

Transoral Endoscopic Modalities: EGD, EUS, and ERCP
Clinical Bottom Line Transoral Modality Anatomical Pathway Primary Output Standard EGD Esophagus -> Stomach -> D2. Direct visualization of the…
-

Risk Stratification for Sedated Upper Endoscopy (2026)
Clinical Bottom Line Risk Parameter Physiological Vulnerability Clinical Modification ASA Physical Status ≥ III Severe systemic disease (e.g., poor ejection…
-

Esophageal Perforation: Mechanisms and Endoscopic Salvage
Clinical Bottom Line Perforation Mechanism Risk Factor Salvage Modality Pneumatic Dilation Achalasia treatment (large 30mm+ balloon). High index of suspicion;…
-

Standard Polypectomy Tooling vs Advanced Resection
Clinical Bottom Line Procedure Class Resection Target Core Instrumentation Cold Snare Polypectomy (CSP) Diminutive/Small polyps (10mm). Submucosal injection needle (lifting…